Lin Jing
Deputy Director, International Oncology WardAssociate Chief Physician
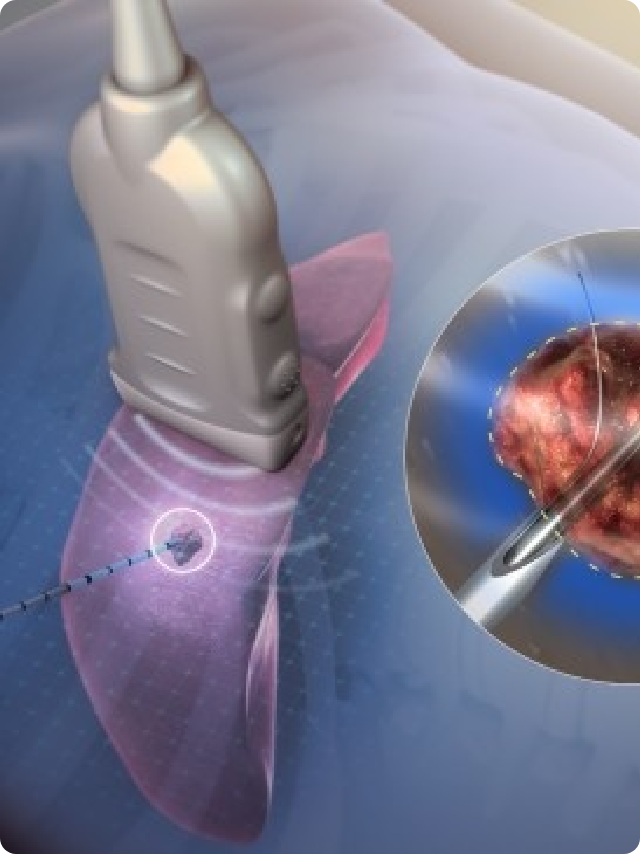
good at professional: Dr. Lin Jing has been engaged in clinical work in oncology for nearly 20 years and is currently a member of the Chinese Anti-Cancer Association. She specializes in minimally invasive targeted therapy, immunotherapy, chemotherapy, radiotherapy and endocrine therapy, and other comprehensive treatments for solid tumors such as breast cancer, esophageal cancer, gastric cancer, intestinal cancer, hepatocellular carcinoma, lung cancer, gynecological tumors, etc. She is also good at gastrointestinal examination, endoscopic jejunal nutritional tube implantation, and endoscopic photodynamic therapy. She is familiar with the principles of various minimally invasive treatments such as intervention, argon-helium cryotherapy, radiofrequency ablation, etc. She is skilled in the prevention of various tumor complications and the diagnosis and treatment of critical illnesses....